

By keeping track of the times you leak urine, you may notice certain times of day when you are most likely to have an accident. You can use that information to make planned trips to the bathroom ahead of time to avoid the accident. Once you have established a safe pattern, you can build your bladder control by stretching out the time between trips to the bathroom. By forcing your pelvic muscles to hold on longer, you make those muscles stronger.
You may notice that certain foods and drinks cause you to urinate more often. You may find that avoiding caffeinated drinks like coffee, tea, or cola helps your bladder control. You can choose the decaf version of your favorite drink. Make sure you are not drinking too much fluid because that will cause you to make a large amount of urine. If you are bothered by nighttime urination, drink most of your fluids during the day and limit your drinking after dinner. You should not, however, avoid drinking fluids for fear of having an accident. Some foods may irritate your bladder and cause urgency. Talk with your doctor about diet changes that might affect your bladder.
Extra body weight puts extra pressure on your bladder. By losing weight, you may be able to relieve some of that pressure and regain your bladder control.
No medications are approved to treat stress urinary incontinence. But if you have an overactive bladder, your doctor may prescribe a medicine that can calm muscles and nerves. Medicines for overactive bladder come as pills, liquid, or a patch.
Medicines for other conditions also can affect the nerves and muscles of the urinary tract in different ways. Pills to treat swelling—edema—or high blood pressure may increase urine output and contribute to bladder control problems.
A pessary is a plastic ring, similar to a contraceptive diaphragm, which is worn in the vagina. It will help support the walls of the vagina, lifting the bladder and nearby urethra, leading to less stress leakage. A doctor or nurse can fit you with the best shape and size pessary for you and teach you how to care for it. Many women use a pessary only during exercise while others wear their pessary all day to reduce stress leakage. If you use a pessary, you should see your doctor regularly to check for small scrapes in the vagina that can result from using the device.
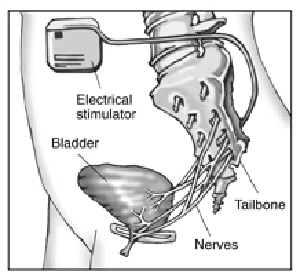
A device can be placed under your skin to deliver mild electrical pulses to the nerves that control bladder function. Electrical stimulation of the nerves that control the bladder can improve symptoms of urgency, frequency, and urge incontinence, as well as bladder emptying problems, in some people. This treatment is usually offered to patients who cannot tolerate or do not benefit from medications. At first, your doctor will use a device outside your body to deliver stimulation through a wire implanted under your skin to see if the treatment relieves your symptoms. If the temporary treatment works well for you, you may be able to have a permanent device implanted that delivers stimulation to the nerves in your back, much like a pacemaker. The electrodes in the permanent device are placed in your lower back through a minor surgical procedure. You may need to return to the doctor for adjustments to find the right setting that controls your bladder symptoms.
Doctors may suggest surgery to improve bladder control if other treatments have failed. Surgery helps only stress incontinence. It won’t work for urge incontinence. Many surgical options have high rates of success.
Most stress incontinence problems are caused by the bladder neck dropping toward the vagina. To correct this problem, the surgeon raises the bladder neck or urethra and supports it with a ribbon-like sling or web of strings attached to a muscle or bone. The sling holds up the bottom of the bladder and the top of the urethra to stop leakage.
Surgery to lift the bladder may use a web of strings (left) or a ribbon like sling (right) to support the bladder neck and urethra.
If your bladder does not empty well as a result of nerve damage, you might leak urine. This condition is called overflow incontinence. You might use a catheter to empty your bladder. A catheter is a thin tube you can learn to insert through the urethra into the bladder to drain urine. You may use a catheter once in a while, a few times a day, or all of the time. If you use the catheter all the time, it will drain urine from your bladder into a bag you can hang from your leg. If you use a catheter all the time, you should watch for possible infections.
Some people with Interstitial Cystitis/Painful Bladder Syndrome find that certain foods or drinks bring on their symptoms. Others find no link between symptoms and what they eat.
Keeping a food diary might help you identify foods that cause flare-ups.
Learning what foods cause symptoms for you may require some trial and error. Keep a food diary and note the times you have bladder pain. The diary might reveal that your flare-ups always happen, for example, after you eat tomatoes or oranges due to the amount of acid that gets into the urine.
If you make changes to your diet, remember to eat a variety of healthy foods.
Bladder retraining is a way to help your bladder hold more urine. People with bladder pain often get in the habit of using the bathroom as soon as they feel pain or urgency. They then feel the need to go before the bladder is really full. The body may get used to frequent voiding. Bladder retraining helps your bladder hold more urine before signaling the urge to urinate.
Keep a bladder diary to track how you are doing. Start by noting the times when you void. Note how much time goes by between voids. For example, you may find that you return to the bathroom every 40 minutes.
Try to stretch out the time between voids. If you usually void every 40 minutes, try to wait at least 50 minutes before you go to the bathroom.
If your bladder becomes painful, you may use the bathroom. But you may find that your first urge to use the bathroom goes away if you ignore it. Find ways to relax or distract yourself when the first urge strikes.
After a few days, you may be able to stretch the time out to 60 or 70 minutes, and you may find that the urge to urinate does not return as soon.
If you have Interstitial Cystitis/Painful Bladder Syndrome, you may feel the last thing you want to do is exercise. But many people feel that easy activities like walking or gentle stretching exercises help relieve symptoms.
Your doctor or nurse may suggest pelvic exercises. The pelvic muscles hold the bladder in place and help control urination. The first step is to find the right muscle to squeeze. A doctor, nurse, or physical therapist can help you. One way to find the muscles is to imagine that you are trying to stop passing gas. Squeeze the muscles you would use. If you sense a “pulling” feeling, you have found the right muscles for pelvic exercises.
You may need exercises to strengthen those muscles so that it’s easier to hold in urine. Or you may need to learn to relax your pelvic muscles if tense muscles are part of your bladder pain.
Some physical therapists specialize in helping people with pelvic pain. Ask your doctor or nurse to help you find a professional trained in pelvic floor physical therapy.
Stress doesn’t cause Interstitial Cystitis/Painful Bladder Syndrome . But stress can trigger painful flare-ups in someone who has Interstitial Cystitis/Painful Bladder Syndrome . Learning to reduce stress in your life by making time for relaxation every day may help control some symptoms of Interstitial Cystitis/Painful Bladder Syndrome .
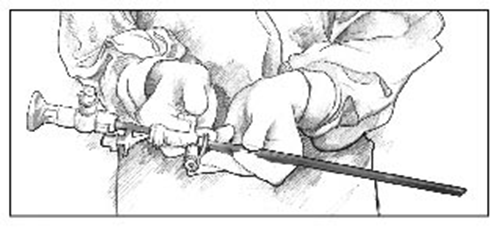
The doctor may stretch the bladder by filling it with liquid after you have been given medicine to make you sleep. Some patients have said their symptoms were helped after this exam.
If you have tried diet changes, exercise, and medicines and nothing seems to help, you may wish to think about nerve stimulation. This treatment sends mild electrical pulses to the nerves that control the bladder.
If you have tried diet changes, exercise, and medicines and nothing seems to help, you may wish to think about nerve stimulation. This treatment sends mild electrical pulses to the nerves that control the bladder.
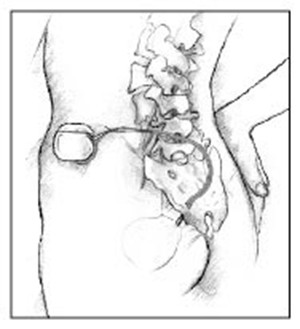
At first, you may try a system that sends the pulses through electrodes placed on your skin. If this therapy works for you, you may consider having a device put in your body. The device works something like a pacemaker, delivering small pulses of electricity to the nerves around the bladder.
For some patients, nerve stimulation relieves bladder pain as well as urinary frequency and urgency. For others, the treatment relieves frequency and urgency but not pain. For still other patients, it does not work.
Scientists are not sure why nerve stimulation works. Some believe that the electrical pulses block the pain signals carried in the nerves. If your brain doesn’t receive the nerve signal, you don’t feel the pain. Others believe that the electricity releases endorphins, which are hormones that block pain naturally.
Implanted nerve stimulation device.
As a last resort, your doctor might suggest surgery to remove part or all of the bladder. Surgery does not cure the pain of Interstitial Cystitis/Painful Bladder Syndrome in all cases, but if you have tried every other option and your pain is still unbearable, surgery might be considered.
Talk with your doctor and family about the possible benefits and side effects.
Points to Remember
This diary will help you and your health care team figure out the causes of your bladder control trouble. The “sample” line shows you how to use the diary.
Your name: ________________________________________________________
Date: ______________________________________________________________
Time | Drinks | Trips to the | Accidental | Did you feel a strong urge to go? | What were you doing at the time? | ||
| What kind? | How much? | How many times? | How much urine? (circle one) | How much? (circle one) | Circle one | Sneezing, exercising |
| Sample | Coffee | 2 cups | X |
| Running | ||
| 6-7 a.m. |
| ||||||
| 7-8 a.m. |
| ||||||
| 8-9 a.m. |
| ||||||
| 9-10 a.m. |
| ||||||
| 10-11 a.m. |
| ||||||
| 11-12 noon |
| ||||||
| 12-1 p.m. |
| ||||||
| 1-2 p.m. |
| ||||||
| 2-3 p.m. |
| ||||||
| 3-4 p.m. |
| ||||||
| 4-5 p.m. |
| ||||||
| 5-6 p.m. |
| ||||||
| 6-7 p.m. |
| ||||||
I used _______ pads today. I used ________ diapers today (write number).
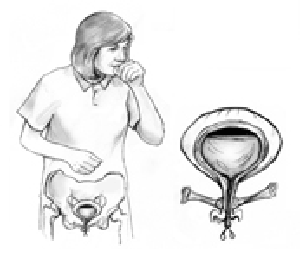
Millions of women experience involuntary loss of urine called urinary incontinence (UI). Some women may lose a few drops of urine while running or coughing. Others may feel a strong, sudden urge to urinate just before losing a large amount of urine. Many women experience both symptoms. UI can be slightly bothersome or totally debilitating. For some women, the risk of public embarrassment keeps them from enjoying many activities with their family and friends. Urine loss can also occur during sexual activity and cause tremendous emotional distress.
Women experience UI twice as often as men. Pregnancy and childbirth, menopause, and the structure of the female urinary tract account for this difference. But both women and men can become incontinent from neurologic injury, birth defects, stroke, multiple sclerosis, and physical problems associated with aging.
Older women experience UI more often than younger women. But incontinence is not inevitable with age. UI is a medical problem. Your doctor or nurse can help you find a solution. No single treatment works for everyone, but many women can find improvement without surgery.
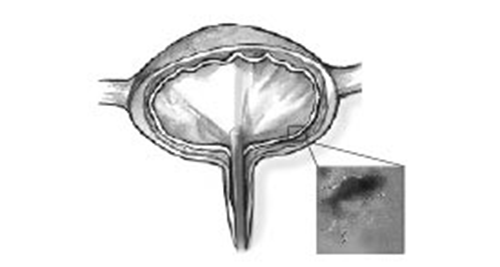
Incontinence occurs because of problems with muscles and nerves that help to hold or release urine. The body stores urine—water and wastes removed by the kidneys—in the bladder, a balloon-like organ. The bladder connects to the urethra, the tube through which urine leaves the body.
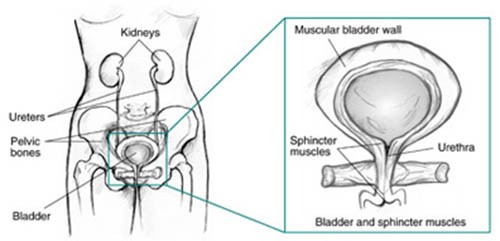
During urination, muscles in the wall of the bladder contract, forcing urine out of the bladder and into the urethra. At the same time, sphincter muscles surrounding the urethra relax, letting urine pass out of the body. Incontinence will occur if your bladder muscles suddenly contract or the sphincter muscles are not strong enough to hold back urine. Urine may escape with less pressure than usual if the muscles are damaged, causing a change in the position of the bladder. Obesity, which is associated with increased abdominal pressure, can worsen incontinence. Fortunately, weight loss can reduce its severity.
Biofeedback uses measuring devices to help you become aware of your body’s functioning. By using electronic devices or diaries to track when your bladder and urethral muscles contract, you can gain control over these muscles. Biofeedback can supplement pelvic muscle exercises and electrical stimulation to relieve stress and urge incontinence.
One of the reasons for stress incontinence may be weak pelvic muscles, the muscles that hold the bladder in place and hold urine inside. A pessary is a stiff ring that a doctor or nurse inserts into the vagina, where it presses against the wall of the vagina and the nearby urethra. The pressure helps reposition the urethra, leading to less stress leakage. If you use a pessary, you should watch for possible vaginal and urinary tract infections and see your doctor regularly.
A variety of bulking agents, such as collagen and carbon spheres, are available for injection near the urinary sphincter. The doctor injects the bulking agent into tissues around the bladder neck and urethra to make the tissues thicker and close the bladder opening to reduce stress incontinence. After using local anesthesia or sedation, a doctor can inject the material in about half an hour. Over time, the body may slowly eliminate certain bulking agents, so you will need repeat injections. Before you receive an injection, a doctor may perform a skin test to determine whether you could have an allergic reaction to the material. Scientists are testing newer agents, including your own muscle cells, to see if they are effective in treating stress incontinence. Your doctor will discuss which bulking agent may be best for you.
In some women, the bladder can move out of its normal position, especially following childbirth. Surgeons have developed different techniques for supporting the bladder back to its normal position. The three main types of surgery are retropubic suspension and two types of sling procedures.
Retropubic suspension uses surgical threads called sutures to support the bladder neck. The most common retropubic suspension procedure is called the Burch procedure. In this operation, the surgeon makes an incision in the abdomen a few inches below the navel and then secures the threads to strong ligaments within the pelvis to support the urethral sphincter. This common procedure is often done at the time of an abdominal procedure such as a hysterectomy.
Sling procedures are performed through a vaginal incision. The traditional sling procedure uses a strip of your own tissue called fascia to cradle the bladder neck. Some slings may consist of natural tissue or man-made material. The surgeon attaches both ends of the sling to the pubic bone or ties them in front of the abdomen just above the pubic bone.
Midurethral slings are newer procedures that you can have on an outpatient basis. These procedures use synthetic mesh materials that the surgeon places midway along the urethra. The two general types of midurethral slings are retropubic slings, such as the transvaginal tapes (TVT), and transobturator slings (TOT). The surgeon makes small incisions behind the pubic bone or just by the sides of the vaginal opening as well as a small incision in the vagina. The surgeon uses specially designed needles to position a synthetic tape under the urethra. The surgeon pulls the ends of the tape through the incisions and adjusts them to provide the right amount of support to the urethra.
If you have pelvic prolapse, your surgeon may recommend an anti-incontinence procedure with a prolapse repair and possibly a hysterectomy.

Side view. Supporting sutures in place following retropubic or transvaginal suspension (left). Sling in place, secured to the pubic bone (center). The ends of the transobturator tape supporting the urethra are pulled through incisions in the groin to achieve the right amount of support (right). The tape ends are removed when the incisions are closed.
Talk with your doctor about whether surgery will help your condition and what type of surgery is best for you. The procedure you choose may depend on your own preferences or on your surgeon’s experience. Ask what you should expect after the procedure. You may also wish to talk with someone who has recently had the procedure. Surgeons have described more than 200 procedures for stress incontinence, so no single surgery stands out as best.
If you are incontinent because your bladder never empties completely—overflow incontinence—or your bladder cannot empty because of poor muscle tone, past surgery, or spinal cord injury, you might use a catheter to empty your bladder. A catheter is a tube that you can learn to insert through the urethra into the bladder to drain urine. You may use a catheter once in a while or on a constant basis, in which case the tube connects to a bag that you can attach to your leg. If you use an indwelling—long-term—catheter, you should watch for possible urinary tract infections.
Many women manage urinary incontinence with menstrual pads that catch slight leakage during activities such as exercising. Also, many people find they can reduce incontinence by restricting certain liquids, such as coffee, tea, and alcohol.
Finally, many women are afraid to mention their problem. They may have urinary incontinence that can improve with treatment but remain silent sufferers and resort to wearing absorbent undergarments, or diapers. This practice is unfortunate, because diapering can lead to diminished self-esteem, as well as skin irritation and sores. If you are relying on diapers to manage your incontinence, you and your family should discuss with your doctor the possible effectiveness of treatments such as timed voiding and pelvic muscle exercises.

Founder of the "IC Aloe Vera"™
![]()
Disclaimer:
These statements have not been evaluated by the FDA and are not intended to be a substitute for professional medical advice, nor is this information meant to diagnose, treat, cure, or prevent any disease. Results may vary.
